Supported by the MyKinergy Platform, Care Navigators are trained, experienced patient advisors that serve as a seamless, cost-effective extension of your clinical team.
At KinergyCare, we go beyond just a technology platform – we believe that people play an important role, too. Research shows that especially for seniors and those with multiple diseases, technology alone may not always be sufficient.
KinergyCare Navigators are a remote workforce that can be economically utilized across facilities, practices, and transitions of care. They are specially trained to coordinate care and act as an advisor or project manager. Care Navigators take on the volumes of non-clinical coordination and follow-up required so that your clinical team can provide skilled care to more patients.
KinergyCare Navigator Benefits
Communication

Lower Cost
Improve Data
Relationships

Satisfaction
Engangement
KinergyCare Navigator Services
Post-Discharge Support
Provide follow-up phone calls after a care transition; decrease “no show” rates at appointments
Education
Assist in accessing community resources; provide health education materials appropriate for patient
Maintain Health Records
Assist to set up and maintain health records in MyKinergy Platform
KinergyCare Navigators view the health care system through the eyes of a patient. They provide patient-centric services that go beyond the walls of a single provider or institution
Next Steps Planning
Create the road map of next steps with family caregivers
Patient and Family Engagement
Use the Patient Activation Measure© (PAM) to assess patient self-management ability; assist patients in identifying own self-care goals; support patient and family caregiver in self-care best practices
Red Flags
Provide earlier identification of “red flags” with use of escalation protocols
KinergyCare Clinical Basis
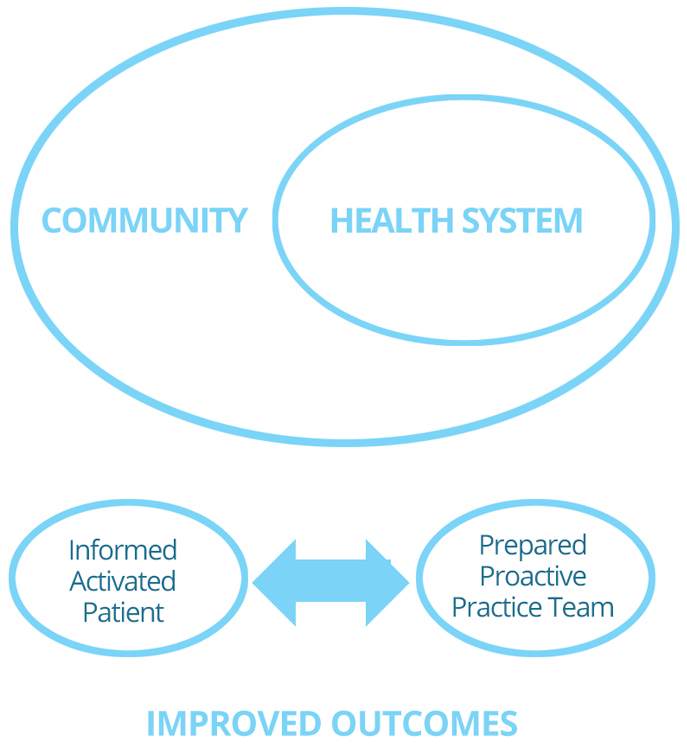
Wagner’s Chronic Care Model
This was developed over a decade ago and now the Chronic Care Model (CCM) is a widely adopted approach to improving care across the health care continuum and has guided clinical quality initiatives in the US and around the world. The authors examined the evidence of the CCM’s effectiveness by reviewing articles published since 2000 that used 1 of the 5 key CCM papers as a reference. The accumulated evidence appears to support the CCM as an integrated framework to guide practice redesign. Redesigning care using the CCM suggests improved patient care and better health outcomes.
Chronic diseases are now the major cause of death and disability worldwide, responsible for 59% of deaths and 46% of the global burden of disease. The CCM is designed to help practices improve patient health outcomes by changing the routine delivery of ambulatory care through interrated system changes meant to make patient-centered, evidenced-based care easier to accomplish.
Goals accomplished through:
a. A combination of Effective Team care and Planned Interactions
b. Self-management support bolstered by more effective use of Community Resources
c. Integrated decision support
d. Patient registries and other supportive Information Technology
These elements are designed to work together to strengthen the provide-patient relationship and improve health outcomes.
Cost-Effectiveness
Evidence on the cost-effectiveness of the CCM is just beginning to emerge, and more research is needed to understand the costs and benefits to practices, payer and patients. A study by <<<et al, states:”External financial incentives and quality improvement support may be essential for widespread practice change.” <<< This is where KinergyCare comes into play. Without utilizing essential practice resources KinergyCare can help take advantage of the CMS incentives.
Evidence of Improved Care
Patients of intervention practices received improved care.
- Compared to patients in control practices, patients of providers actively participating in the congestive heart failure (CHF) collaborative were more knowledgeable, used recommended therapies such as lipid-lowering and angiotensin-converting enzyme (ACE) inhibition therapy more often, visited the emergency department (ED) less often, and experienced 35% fewer days in the hospital.
- When their practices redesigned care according to the CCM, patients with asthma were more likely than patients whose practices did not redesign care to monitor their peak flows and have a written action plan, and their quality of life improved.
- Also, diabetic patients experienced reduced risk of cardiovascular disease; for every 48 patients who received care from a redesigned practice, risk declined by one cardiovascular disease event.
Coleman’s Care Transitions Model
Based on the research done by Eric Coleman, et al. Patients with complex care need who require care across different health care settings are vulnerable to experiencing serious quality problems. A care transitions intervention designed to encourage patients and their caregivers to assert a more active role during care transitions may reduce rehospitalization rates. A randomized controlled study over a years time was conducted, providing either the intervention or the usual course of care. Patient were 65 years or older with 1 of the previously selected conditions.
Intervention patients received the following:
a. Tools to promote cross-site communication
b. Encouragement to take a more active role in their care and to assert their preferences
c. Continuity across settings and guidance from a “transition coach”
Rates of hospitalization were measured at 30, 90 and 180 days. Results showed intervention patients had lower rehospitalization rates at 30 days and at 90 days than the control subjects. The mean hospital costs were also lower for intervention patients ($2058) versus the controls ($2546) at 180 days.
Coaching chronically ill older patients and their caregivers to ensure that their needs are met during care transitions may reduce the rates of subsequent rehospitalization.
The intervention is based on the 4 pillars: (1) Assistance with medication self-management, (2) A patient-centered record owned and maintained by the patient to facilitate cross-site information transfer (3) Timely follow-up with primary or specialty care, and (4) A list of “red flags” indicative of worsening condition and instructions on how to respond to them.
They were operationalized through 2 mechanisms: (1) A Personal Health Record and (2) A series of visits and telephone calls with a transition coach, supporting use of Red Flags, support for medication adherence and increased patient activation through individualizing the setting of SMART goals.
Hibbard’s Patient Activation
Patient activation is a term that described the skills and confidence that equip patients to become actively engaged in their health care. Health care delivery systems can utilize Patient activation to improve patient outcomes and influence costs. The article examines the relationship between patient activation levels and billed care costs. They found patients with the lowest activation levels had predicted average costs that were 8% higher in the base year and 21% higher in the first half of the next year than the costs of patients with the highest activation levels. Knowing patients’ ability and willingness to manage their health will be a relevant piece of information integral to health care providers’ ability to improve outcomes and lower costs.
Activation involves 4 stages:
1. Believing the Patient role is Important
2. Having the Confidence and Knowledge necessary to take action
3. Actually taking action to Maintain and Improve one’s Health
4. Staying the course even under stress
Levels of Activation
Level 1 – Disengaged and overwhelmed – Individuals are passive and lack confidence. Knowledge is low, goal-orientation is weak, and adherence is poor. “My doctor is in charge of my health.”
Level 2 – Becoming aware, but still struggling – Individuals have some knowledge, but large gaps remain. They believe health is largely out of their control, but can set simple goals. “I could be doing more.”
Level 3 – Taking Action – Individuals have the key facts and are building self-management skills. They strive for best practice behaviors, and are goal-oriented. “I’m a part of my healthcare team.”
Level 4 – Maintaining behaviors and pushing further – Individuals have adopted new behaviors, but may struggle in times of stress or change. Maintaining a healthy lifestyle is a key focus. “I’m my own advocate.”
Because the measure is developmental, interventions could be tailored to the individual’s stage of activation. For example, those at early stages of activation would need interventions designed to increase knowledge about their condition and their treatments. Patients at later stages would need interventions designed to increase their skills and confidence in the different self-management tasks. As patients advance in activation, the type of interventions that will be helpful to them will also change. The approach is economical because it is targeted rather than omnibus.
KinergyCare has the PAM as a Key Component of our Care Navigator training, metrics and our priorities of Safety, Defining the Care Navigator Role, Disease Specific Support, Community Resource Involvement and Excellence in Customer Service.